Here is where the science becomes personal.
Within the TAS2R family, one gene has received particular attention from researchers: TAS2R38. It encodes a receptor specifically sensitive to certain bitter compounds, most notably a chemical called PROP (6-n-propylthiouracil) and its close relative PTC (phenylthiocarbamide, a synthetic bitter compound chemically similar to toxic substances found in some plants). What makes TAS2R38 significant is not just what it detects, but how differently it performs from person to person.
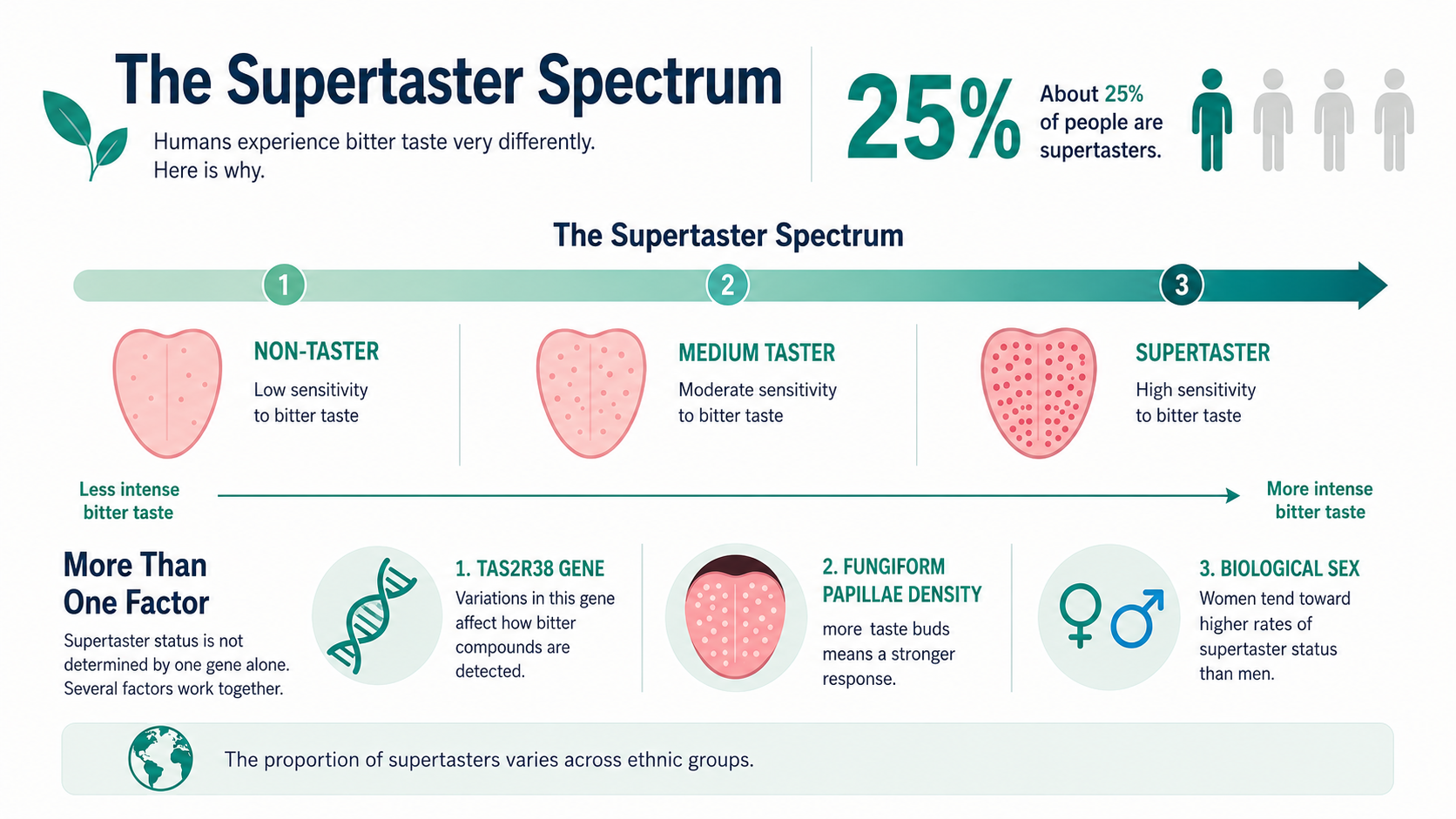
Depending on which variants of TAS2R38 you inherited, you will fall somewhere on a spectrum. Early research mapped these haplotypes systematically, showing how specific genetic variants determine whether a person is a non-taster, a medium taster, or a supertaster. (A haplotype is simply a package of DNA variations that sit together on the gene and are inherited as a group. You get one copy from each parent, and the combination is what places you on the spectrum.)
At one end are non-tasters, people for whom PROP registers as little more than a faint, almost imperceptible bitterness. At the other end are supertasters, people for whom the same compound lands with an intensity that is neurologically in a different category altogether. Not stronger in the way that a louder noise is stronger, but different in the way that a sound heard at normal volume differs from the same sound played directly into the ear.